Be yourself; Everyone else is already taken.
— Oscar Wilde.
This is the first post on my new blog. I’m just getting this new blog going, so stay tuned for more. Subscribe below to get notified when I post new updates.

Who's in your biome?
Be yourself; Everyone else is already taken.
— Oscar Wilde.
This is the first post on my new blog. I’m just getting this new blog going, so stay tuned for more. Subscribe below to get notified when I post new updates.
Humira is the brand name of the drug, adalimumab. This up and comer is an immunosuppressive drug, specifically a monoclonal antibody. We often think of an antigen as only having one antibody, like a married couple. But, it’s more like antigens have multiple partners. This occurs because there are multiple epitopes (peptides or some molecule) on a single antigen. When researchers are trying to develop antibody drugs, they want to isolate a single antibody. A single antibody can be put through experimental tests and expect to give consistent results; whereas, if you have many types, and the composition each time is different, experimental results will change, too. What scientists have figured out is that by isolating a single type of antibody-producing B-cell, a single antigen-specific antibody can be isolated. These B-cells are fused with myelomma cells which are plasma cells that have gone bad (mutations). They can live indefinitely and provide the machinery that the B-cells of interest can use to make antibodies. These are then a serum that has a definite result.
Adalimumab is an antibody that specifically binds to tumor necrosis factor alpha (TNF alpha). TNF alpha is responsible for stimulating the inflammatory response. Chronic inflammation in autoimmune diseases such as rheumatoid arthritis and Crohn’s disease can lead to major issues in joints and intestines respectively. This monoclonal antibody binds TNF which renders it useless. In this way, the antibody can help reduce inflammation throughout the body.
HUMIRA can cause serious side effects, including (This detailed list was found on the hyperlinked website):
Call your doctor or get medical care right away if you develop any of the above symptoms.Common side effects of HUMIRA include injection site reactions (pain, redness, rash, swelling, itching, or bruising), upper respiratory infections (sinus infections), headaches, rash, and nausea. These are not all of the possible side effects with HUMIRA. Tell your doctor if you have any side effect that bothers you or that does not go away.
As will be described in the next chapter, Humira block TNF alpha. TNF alpha is a protein with complex effects. Yes, it is involved in inflammation but it has other roles, too. This is why there are so many possible side effects associated with this drug.
It must be reiterated that the drug is an immunosuppressant. It affects the ability of the immune system to protect you innately and specifically. If you are taking Humira, be sure to consult your doctor. It will increase the chances of getting infected by different bacteria and fungi. TB, specifically, is brought to attention on the website. There isn’t any information on exactly how you become more susceptible, but I can guess. I know that even though a drug has one effect (the one you’re taking it for), it certainly might have others, too. Perhaps it does not only attack (bind) to TNF alpha to reduce inflammation, but also affects other aspects of the immune response. However, suppressing the inflammatory response by itself is deadly. Inflammation is part of both the innate and adaptive response (it itself isn’t specific but can be triggered or enhanced by cells of the adaptive immunity). In this case, TNF is largely secreted by macrophages and monocytes. It acts as a signal for inflammation, but it also has a rule in controlling apoptosis and other mechanisms. Therefore, taking this drug will cripple your immune response and make it more likely to get infections (primary or latent).
The virus continues to spread in certain countries, yet has begun to taper off in others. It remains important in developing accurate tests for the virus. Currently, patients suspected of being infected with the virus will undergo a test that looks for viral RNA, using PCR. PCR amplifies these little molecules to detectable quantities. However, it is vital now that we develop a serological assay to detect a virus. Serological assays detect proteins, and in this case, antibodies.
The CDC continues to suggest that currently developed serological assays must be tested in the lab. If a assay fails to be validated but put into use, it will deliver erroneous information. This could lead to misjudged patient tracking. The necessity therefore lies in the necessity to track previously infected patients, especially those who are asymptomatic. In this way, we can target regions that have higher case loads and implement the necessary measures. These tests will help determine that rate of spread in communities, too. Furthermore, once a vaccine has been developed, it is vitally important to have these assays to test the efficacy of the vaccine to produce an immune response.
In a yet-to-be peer-reviewed paper (though may have large implications), it was shown that detectable concentrations of antibodies only appear 10-15 days after the initial infection. This is to be expected as the immune response (B cell clonal replication) takes about two weeks to work. More surprisingly, it was shown that patients who only had mild symptoms, showed a low percentage of antibody production, specifically neutralizing antibodies. One implication is that there is another component to the immune response then just neutralizing antibodies. This could be antibodies that mark cells for phagocytosis. It also puts to question the efficiency of serological assays. If they are to be effective, we must develop highly sensitive tests or find other proteins involved in the immune response to test. Good luck scientist! We’re counting on you!
With cancer rates increasing, largely due to longer life expectancy and increased exposure to mutagenic factors, there is ever the need to find more effective, less invasive, and far less destructive treatments. Before a tumor has metastasized, doctors may be able to remove the tumor to prevent its spread, but it is an invasive procedure. Furthermore, it doesn’t necessarily stop the spread of the cancer (if it happens to metastasize). Another option, especially if the cancer has begun to spread through the body via the blood or lymph, may be chemo or radiation therapy. However, both of these treatments act to kill fast multiplying cells and aren’t selective against non-cancerous cells.
Low and behold, a new treatment is on the front. Patient specific T-cell therapy. A recent paper suggests modifying T-cells to attack cancer cells specifically. Tumor cells express a series of novel genes that aren’t expressed in normal cells. These tumor cells have a specific peptide sequence due to the accumulation of mutations in these cells. The researchers used these peptides to trigger the clonal response of polyclonal T-cells from patients with cancer. They used patients with medulloblastoma. The brain tumor is very dangerous, and current treatment have proven inadequate in treating high-risk patients. Furthermore, conventional treatments cannot be amplified in this region due to high risk of brain damage.
This method of therapy is being adopted for other types of cancer, too. Researchers are testing the effectiveness of “pulsing” T-cells. It is similar to the method described above. Exposing an array of T-cells to different antigens from different types of tumors reveals the possibility of personalizing T-cells treatment to treat cancer. It’s unfortunate that cancer is becoming more prevalent; however, if we are to continue to proceed with our current lifestyles, we must learn to protect it. And, certainly we’re not going to let some cancer get us down, right?
**This blog is written from a privileged individual, though I’m having some financial difficulties with losing my job, I will be OK thanks for my family ties. My heart goes out to all who are suffering emotionally, physically, financially, etc. due to Covid 19. I hope their stories are getting out, being heard, and received.
Now, here, within and without, we have an opportunity to rest in our thoughts, relish what a simpler life might be like, and find yourself amidst this frozen world. When I’m busy at work, tirelessly writing for school, and squeezing in everything else I really want to do, I find myself far too exhausted and bewildered to settle into my thoughts.
Now, I’m consumed by them, oscillating between the good and bad. In quarantine I’ve found being self-centered excusable, perhaps necessary. Adding to the discord, since being back home my sister was maliciously attacked by her “boyfriend”, friends of friends have died, loved ones have lost dream jobs, I’ve lost the one I love. Though from my hands, the world has been introduced to my first proper shirt and bamboo wind chimes (PLEASE SEE photos — I mean MEME — BELOW!!!). Odd fucking times! Can I say I love it? I prefer it to the last year of being in school, this thing that once seemed so important and interesting. I’m disenchanted. I find it to be a facade yet it is the great pursuit of the American, the stepping stone to recognition, and the guiding principle of society (God might truly be dead!) – I speak to the shape school has taken and the pompous patrons, of course there remains value in it (But what potential for a greater schooling system!). How much life have we lost pursuing what other people deem important!

Here, there is a revelation. Escaping from that which I loathe, leaves an empty space! I’m glad to be reminded! I used to think that living with Mama Nature, perhaps farming or a homestead, that that escape would bring contentment (tried it on a farm in China for a month). Contentment, once realized is a solid rock that will carry you through this life. Yet, it is so variable, no? As I write this, I see the problem. On one hand, I want to be content where I am, by my own doing, and understand that it is merely a mindset. Take the left hand though, it never wants to be content but with what deserves it. That’s all a bit nonsensical. I’ll conclude the thought here. Fuck being always content. Discontentment is the great motivator, fueling change personally and socially; it keeps my body moving. That’s why I can’t feel at home; that’s why I’ll always fluctuate between joy and sorrow. Hope it all ends on a good note!
Within and without I see hope and despair. Hope for a new drive to kick butt, for societal change. Despair in the inevitable revert back to being “content” with normal life and in the moments of sorrow until I meet joy again. Nonetheless, I’m overjoyed with the new green of the trees and the warm weather! I’m excited to meet new people! And, I’m happy to study from home, where I can arrange my time to fit in all extracurricular activities 🙂
Good Luck All!
Perhaps the most detrimental of the sexually transmitted diseases, HIV, has been a long standing pandemic since as early as the 70’s or 80’s. Now, that’s retro! And, so is HIV. It’s retro, a retrovirus. It doesn’t mean this fellow is kicking it back old-school; in fact, due to HIV’s replication mechanism, it continues to be new and improved (though sometimes not improved) via genetic mutations. Retroviruses contain RNA which upon entering a host is translated into DNA, reverse to the “normal” direction of replication (DNA>RNA>protein). According to a paper in Science, this process in HIV involves what is called a intasome, a nucleoprotein complex. They investigated the effectiveness of second-generation HIV integrase strand-transfer inhibitors. The drug is thought to bind to the protein complex but it is not well understood. An issue that has been arising is changing binding sites on the protein complex due to mutations. HIV is an ever-changing virus and as you can see, scientists will have to continue to develop new drugs to fight it back.
For that reason and not being a scientist myself, I believe an important way to alleviate and potentially eradicate HIV is education. One such study shows that persons coming from regions with less HIV education, or perhaps insufficient testing equipment, by a greater percentage are unaware of being infected by HIV. This is likely the biggest factor in spreading the virus. If you don’t know you have it, then no need to inform your sexual partner… But, perhaps it is better to be tested after each new sexual partner, unless you feel you can trust their answer. Condoms help, of course, but so does not having sex. And, frankly neither sound desirable. There is also monogamy… Like, it’s there and it’s a word, but maybe leave it at that. Anyway, free testing should be available to all and easily accessible. Self-test kits should be readily available, too, and ordering them by mail should be an option. Unfortunately, HIV has a bad stigma to it, and that prevents some folks from getting tested in public places.
Science Direct published a paper that shows the increased risk of contracting HIV for those who have herpes simplex virus type 2 (genital herpes). Herpes causes ulcers on genitalia. It is apparent how open sores would increase the risk of contracting HIV, a disease transmitted through bodily fluids or blood. However, herpes also causes an increase in the concentration of immune cells in the genitalia. This is beneficial for the infected individual in lessening frequency and/or severity of reoccurring ulcers. HIV targets these types of cells though, and as herpes causes a sustained increase in regional immune cells, it is more likely to contract HIV if you have herpes. This is just another example of why education and testing are so critically important in reducing the spread of the virus. With this knowledge, one would likely be more cautious when having sex, especially if infected with herpes. Education further acts to reduce the stigma of BOTH of these viruses. I think for Americans, sex is often an awkward topic (likely due to our Christian origins). Since sex is awkward for many, almost impure, any disease associated with it is inherently impure, too. The solution is simple, though, I believe. For the next generation of Americans, let us replace all of the violent and meaningless TV shows and films with ones full of love and sex. Our children will then grow up feeling free to love anyone they want and express that, in one of many ways, with sex. Sexually transmitted diseases will then take their seat next to chicken pox, leaving all stigmas behind. And, people will feel comfortable to ask their partners about these diseases for the sake of health and not disregard it to avoid awkwardness.
Akin to many outcomes of human innovation, we’ve managed to run antibiotics back into the ground within a mere century. Penicillin was the first great gift of mother nature to mankind, an antibiotic synthesized by some mold to wage war against bacteria. Why she decided to bestow anything upon us is a mystery, perhaps it seemed the quickest way to rid this holiest and greatest of plagues from this earth. And, well, it just might be the outcome. Antibiotics provided a way to prevent the worst phenomena, human suffering; and, in doing so, allowed us to continue our pursuit of happiness, also know as suburban life, full of all the gadgets and gizmos of convenience. So, what are antibiotics and how have we managed to turn a blessing into potential extinction?
It wouldn’t be wrong to call antibiotics the weapons of warfare of the microbial world. Life is about surviving, no matter how big or small you may be. We, or they, survive by acquiring the necessities of life. But, they, or we, have the same requirements for life. Inevitably, these circumstances demand competition, even in the highly intellectual homo sapiens, competition continues to be rampant. Don’t worry though, it’s all natural, 100% organic real life. I digress. Little organisms utilize different types of molecules (proteins, nucleic acids, lipids) to either inhibit or destroy fellow competitors to ensure that their own species can get what they need. Alexander Fleming was the first to realize this and consider its potential use. With time, scientist figured out how to produce these antibiotics in large quantities, and there began human’s use of tens of thousands of years of evolutionary development to fight off infection. First used against Staphylococcus, penicillin was then modified to fight off different species and strains of bacteria, and other types of antibiotics were discovered, too.
As described in a paper investigating antibiotic abuse, bacteria, like any other organism, are subject to mutation. These mutations can confer a resistance to some particular antibiotic, and if that be the case, this new strain will survive better and propagate… you know, evolution. Two facts may escape those without knowledge on this matter: bacteria breed like rabbits… times a million, in a matter of hours, you may have millions of bacteria on hand (or agar plate); also, bacteria are capable of transferring genetic material, like telling your friend a cheat to win at cards or dice. Skipping over almost a hundred years, we’ve misused and abused these antibiotics to the point where many of these bacteria are becoming resistant to all available antibiotics. This is a natural process — the development of resistance — but we’ve sped up the affair exponentially. To name a few reasons for this development, antibiotic prescriptions are often halted by the patient before finishing the dose or not taking them in a timely manner; antibiotics are used in livestock feed to promote growth (and prevent disease), which then comes out in manure and so entering our fertilizers and ground water; additionally, antibiotics are used for viral infections, yet these medicines specifically fend of bacteria and are innately ineffective against viruses.
One such bacteria that has developed resistance is Escherichia coli. A study showed that E. coli have now become resistant to fosfomycin. This antibiotic is considered broad-spectrum, meaning that it is effective against many types of bacteria. E. coli, however, has begun to synthesize a molecule that deactivates fosfomycin, called extended-spectrum β-lactamases. Not only has E. coli developed resistance against other drugs, but many other organisms are becoming antibiotic-resistant as well.
To compound the issue, a recent study showed that bacteria like to grow on another byproduct of human kind’s convenient lifestyle, plastic. What are called microplastics, small building blocks of the plastics you’re familiar with, and some that you’re not so familiar with, have found their merry way into the oceans of our planet. They travel mainly through groundwater to rivers, from rivers to the seas. The small deposits come from plastic pollutants and synthetic materials used for clothing that wash off in the washing machine. The researchers investigated the prevalence of “superbugs” on these microplastics relative to uncontaminated water. It seems that plastic offers bacteria a place to attach and grow and form biofilms (essentially thick, mucous films that bacteria secrete).
In conclusion, our conveniences of life, fat cows, cheap clothing, and plastic bags (often used ONLY to carry groceries from the store to your car one time), are unbeknownst to many fostering a mortal enemy.
Polio-my-anus. The world has come together to form a great and altruistic cohort in hopes that Polio won’t leave anyone’s anus ever again. It’s a special thing to see many global leaders working to eradicate poliomyelitis. A testament to what we can accomplish in unity, and a revelation of our stubbornness and failure to tackle other issues together. Nonetheless, this truly is the endgame against polio, as several months ago polio type 3 was confirmed to be globally eradicated. Type 2 saw its last days many years ago in 1999.
For many years, it was debated as to which type of vaccine was better, the inactivated polio vaccine (IPV) or the oral polio vaccine (OPV), and how they worked together. IPV is effective at preparing the immune response in the blood stream when given in several doses, yet it doesn’t activate mucousal immunity so there is a risk of shedding the virus through fecal matter. In addition, it doesn’t present the risk of reverting back to a viral agent. OPV, on the other hand, as it is an attenuated virus, may mutate and regain its “neurovirulence”. The oral vaccine is cheaper and easier to administer, though, and in activating the mucousal immunity, helps reduce the risk of fecal transmission. I find the OPV vaccine quite interesting; it’s like a double-edged sword. Since the virus continues to replicate in the host, when it spreads via water-contamination or the like, it can confer immunity to others. There is danger, though, present in populations with low immunity because the attenuated virus can continue to spread to susceptible hosts. The longer it lives, the more mutations it can acquire, and consequently the more likely it is to reestablish its armory. And, that is the source of circulating vaccine-derived polio virus (cVDPV). Fortunately, a recent study, referenced in an article by The Scientist, showed that OPV and IPV supplement each other. This information comes in a timely manner as the world preps for the final battle against polio virus.
In a meeting at the World Health Organization (WHO) headquarters, the Emergency Committee presented worrisome data. Afghanistan has seen a rise in cases of wild-type polio virus type 1. Due to the current state of affairs in that country, it has proven difficult to administer vaccines to certain regions. Two major issues are people refusing to accept vaccination and a government’s less than wholehearted commitment to the cause. I was surprised to hear that citizens were refusing the vaccine. The committee didn’t mention any potential reasons in the article, and I find it hard to believe that they heard about the vaccine scare in the States. However, if I wasn’t informed on how vaccines worked, I may, too, be frightened by the idea of injecting or drinking (eating?) a virus. The WHO hopes to influence the outcome for the better with financial and emotional support. In any case, we have a real-life, epic story unfolding before our eyes, and perhaps it is not as exciting as Marvel’s Endgame, but not even Captain America could fight off polio virus type 1 without a vaccine! And, that’s the truth.
Microbiomania! Oh sweet and gullible America, an apple-a-day keeps the doctor away! Eggs have too much cholesterol; avocados have belly-burning fats; chocolate is chalked full of antioxidants; coconut oil simply cures all ailments; and, don’t get me started on raw, unfiltered apple cider vinegar (Bragg’s**)! Well, buckle up ladies and gentlemen, the hottest new craze is here: the microbiome! Today, you can’t help but to come across the headline, “new scientific study shows/proves…” when surfing the web or listening to the news. Science is slowly becoming America’s new g(G)od so it makes sense to use it for sales or hype. Anyway I’m here not to talk about misguided beliefs and overly complicated ….; instead, I want to look at the microbiome, discuss briefly the claims and some studies being done.
First, a short description of this tiny world. According to the National Human Genome Research Institute, the individual is more a vessel for microbes than it is construction of genome-encoded human cells. There are far more microbial cells in the human body than there are human cells. Perhaps this comes as a surprise; yet in studying evolution and ecology, it is clear that many environmental niches exist internally and externally in and on the human body. Throughout the planet, environmental niches, as a rule, will be filled with life. There may be a few exceptions, but we even find life in seemingly inhospitable places, in hot, cold, salty, acidic, toxic, you name it, places. Therefore, it is reasonable that a place of both organic and inorganic materials, moderate temperatures, and a variety of pH levels, would thrive with life!
Following this train of thought, the discovery of how codependent these organisms have become, to the extent that one may not live without the other, should come with a: “oh, of course! That makes sense!”. The Harvard School of Public Health informs us that certain vitamins and amino acids are synthesized by the microbiome. In addition, the human metabolic system is unable to digest certain foodstuffs, yet the microbiome can and does, with some of the byproducts further serving our health and functionality. Even their mere presence creates competition that works to defend the system against potentially pathogenic microbes.
One study investigating the composition of the microbiome during pregnancy and lactation, and the effects of commonly used (during pregnancy) anti-depressants on the microbiome, shows an important byproduct of microbes, tryptophan, used in the synthesis of serotonin. Serotonin, 95% of which is found in the GI tract, is an important neurotransmitter in human physiology and low concentrations of it have been linked to depressive disorders. They showed, using mice as a model, that serotonin levels are disrupted by abnormal microbe communities. It was also shown that anti-depressants, such as fluoxetine, disrupt the microbiome. The implications of this are important to consider. Infants are immunocomprimised in part due to an immature microbiome. Though environmental exposure has a part, the microbes acquired by the infant’s journey through the vagina and by breast milk, have a crucial role in its establishment. If the mother’s microbial community is compromised, it may directly affect not only the newborn’s microbiome but consequently its ability to ward off disease causing microbes.
The significance of the microbiome on human health, and its potential use in the medical world are apparent. What becomes difficult in these early days of research, is the extent of our ability to manipulate it and in an informed way. For instance, an investigative study of oral probiotic supplements’ effects on vaginal microbiota, returned inconclusive results. In comparision to a negative control, post-probiotic vaginal microbiomes remained similar to the control and baseline. It is possible the normal microbiome is resistant to manipulations, or, that given orally these probiotics are inneffective. It is important to realize that there are many facets of the microbiome that have yet to find a consensus among researchers.
All this to say, beware! Follow basic guidelines to a healthy life, diverse diet (excluding garbage), exercise, laugh, and sleep well. Certainly the investigations of the human microbiome will yield some insights but be patient! If I could suggest one thing, it’d be to keep a sample, from a healthy donor, of fecal matter just in case you are colonized by Clostridium difficile. Fecal transplants have been shown to be 80-90% effective against C. difficile infections. And, it’s easy! Just like pooping but in reverse!
According to a paper submitted to the Public Health Report, influenza pandemics have been occurring for at least the past 500 years. A number of influenza pandemics have plagued the planet over the past century, most notably the Spanish flu (1918 pandemic), which saw the H1N1 strain as the culprit of roughly 50 million deaths. Today, influenza virus, with its numerous strains, still circulates the globe. I suspect its prevalence and ability to readily cause epidemics and pandemics, in part, is due to population density. Since the onset of towns and cities and the accompanying close quarters habitation, diseases, whether by bacteria or viruses or parasitic insects, have been transmitted more readily and easily.
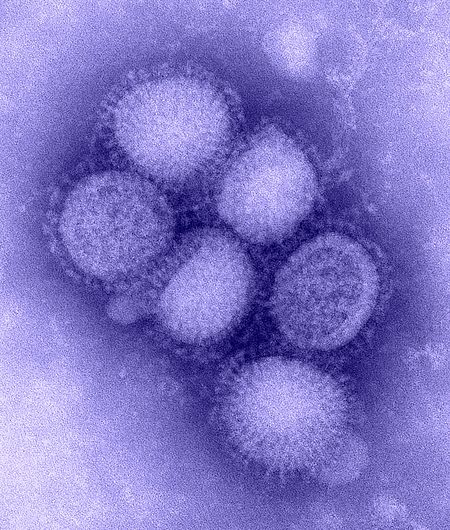
Influenza is generally transmitted through the air and proceeds to infect the upper respiratory tract. Two virulence factors contribute to the virus’s annual ability to evade vaccines. Their envelope contains two proteins, each of which has different variations. The CDC states that different combinations of the surface proteins make it nearly impossible to concoct a single, effective vaccine; furthermore, as it is a RNA virus, gene replication is prone to mutations which effects the structural make-up of the proteins and the human’s immune response to neutralize it. Humans aren’t the only reservoir either, influenza A also infects other animals. It is these strains of the virus which pose potential pandemic outbreaks. They don’t normally infect humans because they don’t have the correct proteins to attach to our cells; however, genetic alterations in their genome may produce new surface proteins that can. After what is called antigenic drift, a mutation in the genome, the virus can infect individuals who are vaccinated, though the virus remains similar to the original and the body’s immune response (post-vaccination) still has some efficacy in fighting it. This is the cause of the seasonal influenza virus, those that typically reside in humans. When antigenic shift occurs, two different strains of influenza exchange RNA molecules. In this way, a virus that previously infected swine, may obtain RNA molecules that encode proteins allowing it to infect humans. It is these novel viruses that often cause pandemics.
Each year, different strains of influenza may be more prevalent than others. Experts in the field monitor influenza circulation throughout the globe to better predict which strains will make an appearance. Dr. John Ross describes how these predictions are made for the northern hemisphere. In Australia, the “flu season” occurs during our summer. By observing which strains affect this great island continent, experts can surmise that these variations will make their way northward for our “flu season”, from autumn to late winter. I guess Australia’s out of luck… To be clear, they are tracking variations of the “seasonal flu” virus and not novel viruses. “Seasonal flu” vaccines, though provide partial protection from antigenic drift varieties, are unlikely to provide a super charged immune response against novel viruses. Instead, the United States government has created a stash of vaccines (“pre-pandemic vaccines”) for potential novel viruses. They are probably tracking these viruses in their respective warm-blooded hosts and conjuring up vaccines in case they undergo an antigenic shift event. If, however, a novel virus, one without a “pre-pandemic vaccine”, makes the jump to a human host, it will take some time to develop an effective vaccine. Six months were needed to deliver the H1N1 vaccine during the 2009 pandemic, and a little over another month to produce large quantities. In case of another pandemic, while you’re waiting for a vaccine to be created, the best way to avoid giving birth to a virus, like with human babies, is to practice abstinence! Don’t touch anyone or speak with anyone and certainly don’t wipe the snot from your human baby’s or grandma’s face! That, or just wear a mask and wash your hands frequently and don gloves… I’ll take my chances with the latex.
Many lessons can be learned from Andrew Wakefield’s poorly designed and fraudulent study investigating a proposed link between the measles virus and Crohn’s (or, is it “… enterocolitis”?) disease, and later, autism. Of the more relevant, who’s funding the research and what are their motives? Not to say that someone should have known Wakefield was being funded by a lawyer who represented JABS, a anti-vac group; he was wise to keep that secret to anyone who would lift a finger. In Brian Deer’s investigative report, it reads clearly that nearly every motive and decision Wakefield made in and around the study (and its accompanying business ventures) was to infect the country with JABSviridae and let its toxin fund his enterprises.
Any good scientist will observe phenomena and make hypotheses, though it’s a stretch to make business models after them. Andrew Wakefield wanted a particular outcome, a link between MMR vaccination and “autism enterocolitis”, so he could provide diagnostic methods, a new single measles shot, and possibly treatment for autism. Perhaps, he really felt there was a link and just sought to make a living off of it, too. But, the fact that he had the lawyer, Richard Barr, seek out children with the proper “signs”, which rules out random selection, and that, the study only included 12 participants, leads me to believe he cared more for his business endeavors.
It’s also curious as to why The Lancet even published the paper. The study was poorly designed, the paper has no concrete conclusions, especially as pertains to the link with autism, and even if they had made some discoveries, it’d be hard to trust the data with so few participants. Eventually, a new head of medicine arrive at the Royal Free Hospital, Mark Pepys, who pushed him to do the study again but properly. Wakefield’s neglect and non-compliance to the push lost him the research position.
Interestingly, a study published in Clinical Infectious Diseases in 1997, before Wakefield’s paper, investigated the safety of multiple different vaccines, MMR, MMRV, and VARIVAX. A total of 812 children were used in the study. Each was given a variation of the aforementioned vaccines and some a placebo. The only undesirable reaction shown were minor rashes, fevers, and sometimes mild cases of chicken-pox. This fact only makes it more confusing why The Lancet and the public believed the outrageous claims made by Andrew Wakefield.
